Childhood cancer survival rates have soared. A new St. Jude study reveals what happens after treatment ends. Medicine hasn't solved it yet.
Why it matters
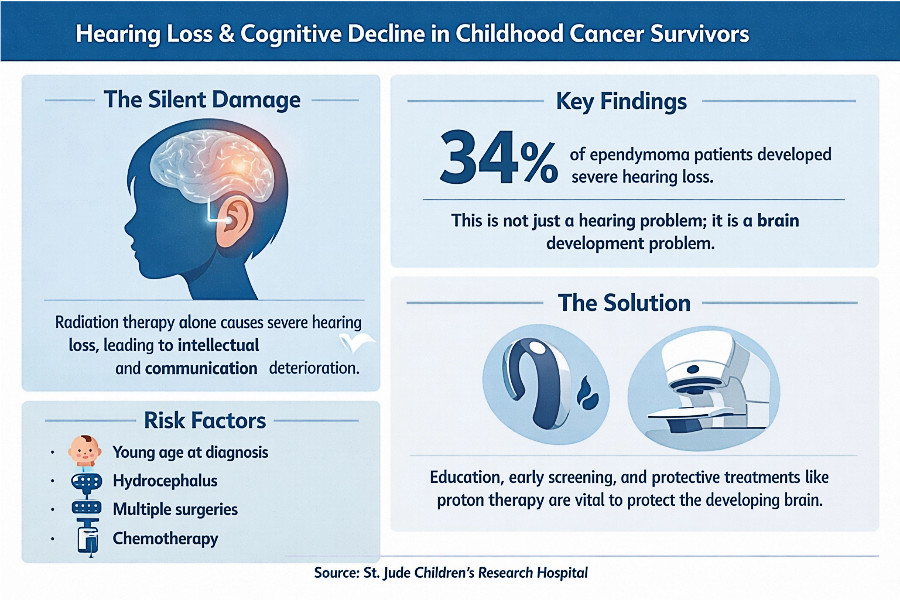
Radiation therapy alone — no chemotherapy required — causes severe hearing loss in a significant share of pediatric brain tumor patients. This is not a hearing problem alone. These are kids whose intellectual development deteriorates because of the treatment that saved their lives. Specifically, intellectual ability and communication skills deteriorate. The damage is measurable, progressive, and tied to the cochlear injury radiation causes.
Assumptions, assumptions
Clinicians long assumed hearing loss required both chemotherapy and radiation to trigger cognitive decline. St. Jude researcher Heather Conklin, PhD, dismantled that assumption: "We saw a high rate of hearing loss and greater cognitive decline, even in a group that only received radiation."
That finding changes the calculus for oncology teams. Radiation-only patients can no longer be treated as lower risk for auditory and cognitive side effects. The screening and monitoring support has to shift.
 Published in Neuro-Oncology, research from St. Jude led by Heather Conklin, PhD, Department of Psychology & Biobehavioral Sciences, demonstrated that radiation therapy was a significant individual contributor to hearing loss, a risk directly linked to cognitive health, in children treated for ependymoma. Photo credit: St. Jude Children's Research Hospital.
Published in Neuro-Oncology, research from St. Jude led by Heather Conklin, PhD, Department of Psychology & Biobehavioral Sciences, demonstrated that radiation therapy was a significant individual contributor to hearing loss, a risk directly linked to cognitive health, in children treated for ependymoma. Photo credit: St. Jude Children's Research Hospital.
By the numbers
-
145 children treated with radiation for ependymoma, a childhood brain tumor
-
34% developed severe hearing loss in at least one ear
-
Children with severe hearing loss showed worse intellectual ability and communication skills, plus a greater decline in intellectual ability over time
-
Verbal learning and memory held. Intellectual ability and communication skills did not. The damage follows a pattern, which means it can be anticipated.
A closer look
Ependymoma patients face a compounding disadvantage. They are younger at diagnosis than kids with other brain tumors, and their tumor location puts the cochlea directly in the radiation's path. Additional risk factors, in order of developmental significance:
-
Young age at diagnosis (intersects with key developmental windows for language and cognition)
-
Hydrocephalus
-
Multiple surgeries
-
Chemotherapy before radiation
Sex, race, and socioeconomic status showed no association with outcomes.
The intrigue
What motivates hearing aid adherence: telling parents the truth. Surveyed parents said they would prioritize hearing aids more if they understood the direct link to brain development. Conklin's team is betting that education, not prescription alone, drives better outcomes.
In other words, the intervention is not just medical. It is informational. Telling parents the truth about what hearing loss does to a developing brain changes their behavior.
The challenge
The tools exist. Consistent use is the problem.
-
Hearing aids, cochlear implants, and targeted academic supports all help.
-
Proton therapy, more precise than conventional photon radiation, can spare the cochlea.
-
Certain medications protect cochlear hair cells during chemotherapy. Discomfort, stigma, and device complexity all chip away at adherence.
The bottom line
Beating cancer is the first fight. Protecting the developing brain is the second. Right now, medicine is losing too many kids to the fallout of their own cure.
For families in the middle of it right now, the question to ask your oncology team is simple: What is your plan to protect my child's cochlea?