Barbara Schmidt, 83, shattered her hip on a driveway. Fell down an escalator in Germany. Knocked herself unconscious decorating for Christmas, bruising her face. Her family feared an illness. The real culprit—and one facing millions of American seniors? Over a dozen prescription drugs were prescribed to help her.
Why it matters
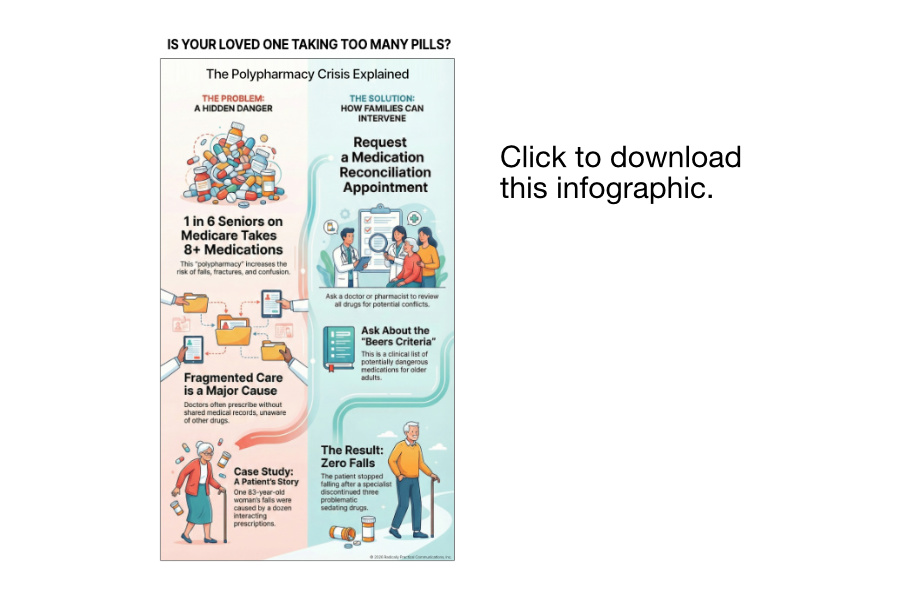
One in six Medicare seniors takes eight or more medications. A Wall Street Journal analysis of Medicare Part D data for 46 million enrollees shows that this polypharmacy crisis causes preventable falls, fractures, and confusion.
By the numbers
46 million seniors are enrolled in Medicare's drug benefit.
-
Schmidt took prescriptions from at least 5 different providers
-
She's had nine surgeries, including hip and knee replacements.
-
Zero falls since stopping three sedating medications in 2023.
However, this is only half the story; the real danger lies in how these prescriptions ended up on her shelf.
The problem
Doctors often prescribe multiple medications without shared medical records. Patients don't always report other prescriptions, and specialists often work in isolated systems. Each treated a specific issue, without considering the combined effect.
Zoom in
Schmidt took three drugs on the Beers Criteria, a widely-used clinical guideline maintained by the American Geriatrics Society that flags potentially dangerous medications for older adults:
-
Diazepam (Valium) for anxiety
-
Hydroxyzine, an antihistamine for anxiety
-
Methocarbamol, a muscle relaxant
She also took gabapentin (900mg daily) for a decade for back pain and trazodone for sleep without a depression diagnosis. All sedate. Together, they increased her risk of falling.
Red flags for families
-
Parent taking 8+ medications from different doctors
-
Increased confusion, dizziness, or balance problems
-
Prescriptions from providers without shared records
Reality check
Medicare requires insurers to provide a comprehensive drug review, but only for a limited subset of patients. Schmidt didn't qualify due to insufficient chronic conditions despite taking over 12 medications.
The Journal found these reviews don't reduce prescription counts.
The breakthrough
A specialized geriatric clinic, arranged by Schmidt's daughter in March 2023, who works in healthcare, to spot the danger. A pharmacist conducted a thorough medication review. Geriatrician George Hennawi told her plainly: these three drugs were causing her confusion and falls. "They all work somewhat the same way," Hennawi says. "Combining all of them is a higher risk for complications."
Schmidt was shocked. No doctor had warned her.
The takeaway
Schmidt stopped the three problematic medications. She now takes hydroxyzine only when stressed, and rarely. She hasn't fallen since. She feels clearer. "I'm better than I was," she says.
Gabapentin? Stockpiled. "I hang on to it in case I might need it. You get old. You don't throw drugs away," Schmidt told the Journal. Schmidt had experienced withdrawal symptoms after stopping her benzodiazepine cold turkey during a hospital stay, which is a dangerous practice that highlights the need for medical supervision when stopping these drugs.
The bottom line
The highest prescribing rates are in rural Southern areas with high chronic disease rates, where some doctors often prescribe eight or more drugs per patient.
This isn't just one patient or region. It's systemic. Millions of seniors pay the price.
What you can do
-
Request a medication reconciliation appointment for elderly relatives taking 5 or more drugs.
-
Ask doctors: "Is this on the Beers Criteria for seniors?"
-
Bring complete medication lists, including OTC drugs, to every appointment.
-
Push for shared electronic medical records across all providers.
► Download the infographic →